
Achilles tendinosis
What is Achilles tendinosis?
Achilles tendinosis describes a painful, degenerative condition affecting the Achilles tendon either at its attatchment to the calcaneum (Insertional Achilles Tendinosis) or a few centimetres above this (Non-Insertional Achilles Tendinosis) . It is helpful to describe it as an imbalance between the perpetual natural breakdown and repair of the tendon.
With age, the collagen fibres that make up the Achilles may become less flexible and weak which explains why these injuries tend to occur in middle-aged athletes.
Small 'micro-tears" in the tendon may occur often as part of an over-use injury. This may result in inflammation and a painful swelling as the body attempts to repair the tendon.
The area just a few centimetres above the heel attachment appears to have a poor local blood supply which is thought to be another predisposing cause of non-insertional Achilles Tendinosis. Some patients are seen to have small areas of new blood supply (neovascularisation) to the deep portion of the tendon which may account for a proportion of pain.

Fig.1. Photograph and Xray of prominent heel bump or ”Haglund” deformity.
Some people have a prominent bump of bone at the back of the heel (called a ‘Haglund deformity or ‘pump bump’) which can impinge on the Achilles attatchment causing an insertional tendinosis. An inflamed pocket of fluid (called a bursa) can also develop between the Haglund deformity and the tendon leading to acute pain and swelling.
Why does Achilles Tendinosis Occur?
As already mentioned there are some causes unique to the individual such as local blood supply, shape of the heel and age!
There are a number of other factors which may account for increased stresses through the tendon, we often call these ‘biomechanical factors’ these include:
How is Achilles Tendinosis diagnosed?
Very often your specialist will be able to diagnose Achilles tendinosis by taking a careful history and examining you, It is not always necessary to perform further investigations but we may arrange for an ultra-sound scan, doppler or MRI scan to assess the degree of tendon involvement.

Fig. 2. Photograph showing the back of the ankle. A. Achilles tendon. B. Achilles insertion. C. Bursa. D. Peroneal tendons.
How is Achilles Tendinosis treated?
The majority of patients with Achilles tendinosis do not require surgery.
The aims of treatment are to:
tendinosis
As with any other type of over-use injury, initial rest from the precipitating cause is helpful to prevent further damage.
Specific exercises called ‘Eccentric stretches’ promote the repair process within the tendon, in much the same way as weight training strengthens muscles.

Fig. 3.1 Eccentric stretches: Standing on a stair, holding on to the handrail throughout, use both calves to raise up on tiptoe.

Fig 3.2 Lift good foot up, off the stair.

Fig 3.3 Standing on one leg, lower the heel to the level of the stair.
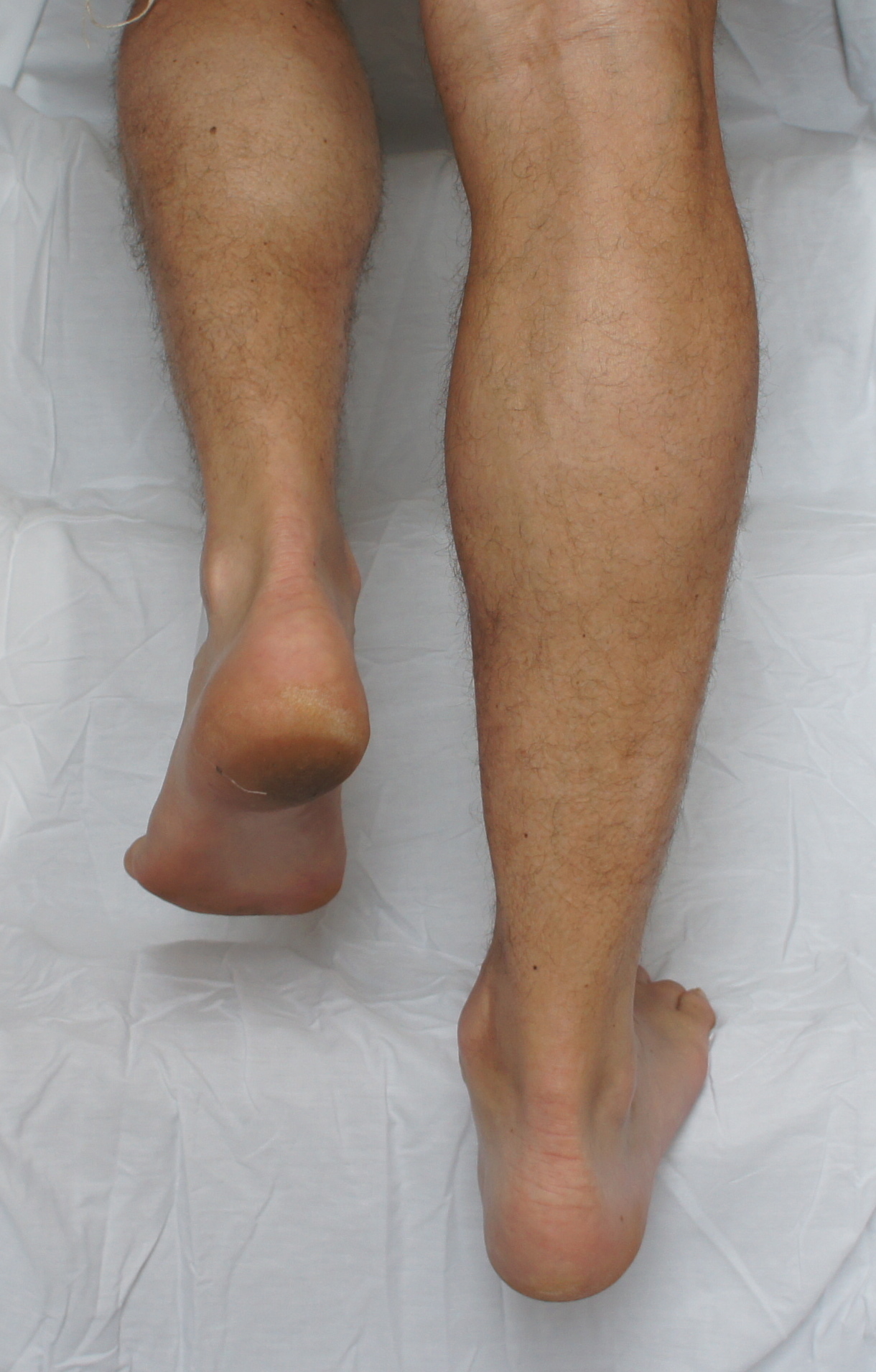
Fig 3.4 lower below the step, and repeat raising up on two feet again.
Fig. 3. Eccentric stretches
Your physiotherapist will concentrate on stretching especially stretching exercises of your calf. They will also assess your general posture, (in some people poor spinal posture can lead to a compensatory hamstring and calf tightness) and might teach you exercises to improve your core strength.
In many patients insoles (orthoses) with a supportive arch can be very helpful in preventing over-pronation which offloads the tendon. A temporary 1cm heel lift may be placed in the shoes to help reduce the final strain on the tendon during walking but should be discarded after two weeks once calf stretches have begun.
Extra-corporeal shock wave therapy (ESWT) is a new treatment that uses sound-waves to stimulate tendon repair in some resistant cases,
Anti-inflammatory tablets may help reduce the pain and inflammation early on.
We do not recommend the use of steroids for Achilles Tendinosis due to the risk of rupture associated with these agents. Similarly there is little evidence to indicate injection of plasma or platelets into the tendon has a positive therapeutic effect.
What does Surgery involve?
Surgery is only advised in those who have failed to improve with non-surgical treatments, this is because surgery carries a small risk of complications.
Non-insertional tendinosis: Surgery is sometimes required in individuals whose symptoms don’t settle with simple non-surgical treatments. Surgery involves a ’debridement’ in which the tendon sheath is opened, and any areas of degeneration within the tendon are removed after which the sheath and skin are carefully repaired. In those with small areas of new blood vessel formation (neovascularization) procedures to strip off the blood vessels are often useful.
A period of 2 weeks in plaster is usually required to allow the wound to heal followed by four weeks of reduced activity accompanied by early rehabilitation with the physiotherapist.
Sometimes, in severe tendinosis or in those with recurrent symptoms a tendon ‘augmentation’ maybe needed. A tendon augmentation involves removing the worst affected part of the tendon and transferring an adjacent tendon (usually the big toe tendon which is called FHL) and fixing it to the heel next to the achilles, to maintain strength. The big toe tendon is rarely missed because another tendon takes over its role.
This surgery is more involved and usually requires 6 weeks of immobilization in a plaster or boot.
Insertional tendinosis:
Again surgery should not be considered unless non-surgical treatments have been exhausted, as surgery carries a risk of complications.
Surgery for insertional tendinosis involves decompressing the prominent bone at the back of the heel (calcaneum) called a ‘Haglund deformity’, that acts to abrade and irritate the tendon, along with the inflamed ‘bursa’.
The Haglund deformity can be removed directly in the case of small prominences the achilles can be left intact with larger lumps the achilles should be lifted off to allow sufficient clearance. see fig below.
Fig4. Before Haglund excision (note previous arthroscopic scar from failed excision
Fig 5. Post Haglund excision.
Fig. 6.Diagram showing elevation of the achilles, removal of the ‘haglund deformity’ and reattachment with an Arthrex ‘suture bridge’
In some cases the prominent Haglund deformity can be rotated away from the achilles by removing a wedge based at the top of the heel bone in front of the achilles and closing the gap, this is fixed with a staple or screw. After this operation.

Are there any risks of surgery?
As with all foot and ankle surgery, surgery to the achilles carries a small risk of complications. As well as the standard risks of infection, wound breakdown, nerve injury and bleeding Achilles surgery carries the specific risk of rupture of the tendon, which is the reason for the necessity of the plaster of paris and careful rehabilitation.
Be sociable..share!
















